

By ANISH KOKA
I used to be listening to a dialog between two essential thinkers I respect drastically: geneticist/technologist/blogger Razib Khan and Washington Put up columnist Megan McArdle. Their dialogue was a freewheeling rant concerning the issues they see with the rise of populism on the left and proper, however a throwaway remark associated to the US doctor scarcity within the context of needing excessive expert immigrant labor in the direction of the top of the virtually two-hour dialog made me understand how little folks actually learn about healthcare in America. In fact, everybody is aware of sure points of healthcare as a client very properly, however even in case you are a high-IQ particular person who could make use of the huge data in any respect of our fingertips, it’s exhausting to actually know what the truth on the bottom is with out residing it / having deep data. Apparently sufficient, early on Megan and Razib each acknowledge the impossibility of commenting on the state of affairs in Iran, as a result of the Iraq struggle taught them the folly of constructing conclusions from the accessible data. Backside line, it doesn’t matter how good you’re in case your conclusions are primarily based on studying Colin Powell on the weapons of mass destruction Saddam Hussein will need to have. The general public could not understand it, however well being coverage has an identical downside. The overwhelming majority of lecturers “overlaying” American well being coverage, and answerable for describing healthcare, are ideologues whose essential objective is to not describe actuality, however to vogue a narrative. And as any screenwriter will let you know — don’t let the information get in the best way of a very good story.
What follows is an examination of what occurs once you pull one of many necessary healthcare threads that kinds the bedrock of many healthcare opinions that good folks like Megan and Razib maintain: Rural entry to healthcare in America.
First, right here’s what a Google search reveals — and spot the sources. I guarantee you that PubMed just isn’t a lot completely different. Rural healthcare entry in America should be dangerous, proper?
As soon as we set up that healthcare entry in rural America is “dangerous”, there are all types of conclusions which are downstream from that like funding of rural hospitals, and administration of the doctor labor provide.
However the unusual factor concerning the rural healthcare entry downside that ought to strike anybody over a sure age that has adopted/lived healthcare is that now we have been speaking about this and passing laws on the matter without end, and but in case you are to imagine those that ought to have probably the most data about this stuff, we proceed to fall brief.
Understanding what precisely is occurring requires some data of the legislative sausage that has created the present panorama. Understanding the legal guidelines and extra importantly how they’re applied ought to rapidly make the reader perceive why there’s a highly effective incentive to take care of a sure narrative.
A short abstract of some main laws at the moment on the books exposes precisely why it could be so necessary to take care of a sure narrative on rural well being care entry.
The Critical Access Hospital (CAH) designation, created by the Balanced Finances Act of 1997 after a wave of rural closures, gave over 1,300 hospitals cost-based Medicare reimbursement — that means Medicare pays regardless of the hospital studies it price to ship the service.
The Rural Health Care Access Act of 2025 (H.R. 771) goes additional, eliminating the space requirement {that a} hospital should be greater than 35 miles from one other hospital to qualify as a CAH, extending cost-based reimbursement to hospitals that had been by no means distant sufficient to fulfill the unique threshold.
The Rural Emergency Hospital (REH) designation permits low-volume rural hospitals to drop inpatient beds whereas retaining emergency and outpatient providers — and receiving further federal funds — with latest laws proposing to increase eligibility to hospitals that closed way back to 2014.
Congress has additionally allotted new Medicare-funded Graduate Medical Schooling (GME) residency slots particularly for rural hospitals, regardless that a December 2025 GAO report discovered that 95 p.c of the hospitals receiving slots had been geographically city hospitals that had legally reclassified themselves as rural to qualify.
The Rural Well being Focus Act formally authorizes the CDC Workplace of Rural Well being with devoted appropriations, and the Honest Funding for Rural Hospitals Act modernizes disproportionate share hospital funds with a $20 million per-state funding ground.
Maybe most consequentially, one of many main political shields in opposition to site-neutral payment reform — the coverage that will equalize Medicare reimbursement no matter whether or not a service is delivered in a hospital outpatient division or a doctor’s workplace — a change that will save Medicare tens of billions yearly comes from these arguing that this alteration would shut a whole bunch of rural hospitals inside six months.
Each one in every of these packages represents a funding line. And each try to shut the loopholes in these packages is rapidly crushed with an avalanche of moralizing about saving cash on the again of the indigent. You’ll be able to perceive that there are a whole lot of pursuits which have a lot to realize by promulgating a rural well being care entry hole. Nowhere is the spin on American healthcare extra apparent than when it falls to lecturers to critique it. Tutorial well being coverage wonks nationally and internationally constantly rank American healthcare as woefully insufficient relative to our peer nations which have some type of nationalized/socialized healthcare.
This narrative has a robust institutional dwelling. The Commonwealth Fund’s Mirror Mirror report, in all probability probably the most broadly cited worldwide healthcare comparability, has ranked the USA final or near-last amongst high-income nations in nearly each version for the previous 20 years. The report’s methodology leans closely on insurance coverage protection, administrative burden, fairness metrics, and survey-based measures of affected person expertise. International locations with nationwide insurance coverage methods — the UK, Canada, and the Nordic nations — rating properly on the entry dimension virtually by definition, as a result of common protection is handled as equal to common entry. The American system, with its patchwork of personal insurance coverage, Medicaid, and Medicare performs poorly on these metrics and will get ranked accordingly. These rankings are then cited in congressional testimony, think-tank studies, and op-ed pages as proof that the American healthcare system is inferior — that People get much less for extra, and {that a} nationwide insurance coverage program would repair it.
However what good is a nationwide insurance coverage card if there is no such thing as a hospital throughout the essential 90 minute time window when you’ve got a coronary heart assault? Insurance coverage protection and geographic entry to care should not the identical factor. A affected person in rural Canada has common protection however could wait hours for an ambulance to achieve a cardiac cath lab — if one is reachable in any respect. A affected person in rural Nevada could also be uninsured and be at a PCI-capable hospital in 40 minutes. The previous is counted as “entry” within the Commonwealth Fund framework. The latter is counted as a failure. The rankings measure the bureaucratic structure of insurance coverage methods, not the bodily actuality of whether or not care might be delivered, particularly when it’s most urgently wanted.
So how about we truly attempt to quantify the American patchwork and examine it to one in every of our peer nations that’s presupposed to be a mannequin for us — our Medicare for All Canadian neighbor.
Percutaneous coronary intervention — the process that opens a blocked coronary artery throughout a coronary heart assault — is near a great proxy for healthcare entry broadly. It’s definitionally time-sensitive: the ACC/AHA guidelines set a 90-minute door-to-balloon goal for a motive, and delays past that threshold carry measurable mortality/morbidity penalties. It requires important infrastructure — a catheterization laboratory, educated interventional cardiologists, a specialised staff accessible across the clock. It’s subsequently not uniformly distributed throughout geographies. And crucially, it’s a process the place now we have wonderful public information on precisely the place it’s being carried out.
Entry to PCI just isn’t an ideal proxy for entry to all medical care. But when a neighborhood has a functioning PCI program inside cheap distance, it virtually actually has the broader infrastructure — emergency providers, hospital beds, superior imaging, specialist protection — that defines a purposeful healthcare ecosystem. The inverse can also be roughly true: communities removed from PCI are usually removed from the remainder of superior care as properly. PCI entry is an inexpensive healthcare canary.
Once you measure the precise distance between the place People dwell and the place the closest cath lab is — utilizing actual hospital information and population-weighted geography — what do we discover?
Constructing the maps — and what they present
How the U.S. map was constructed
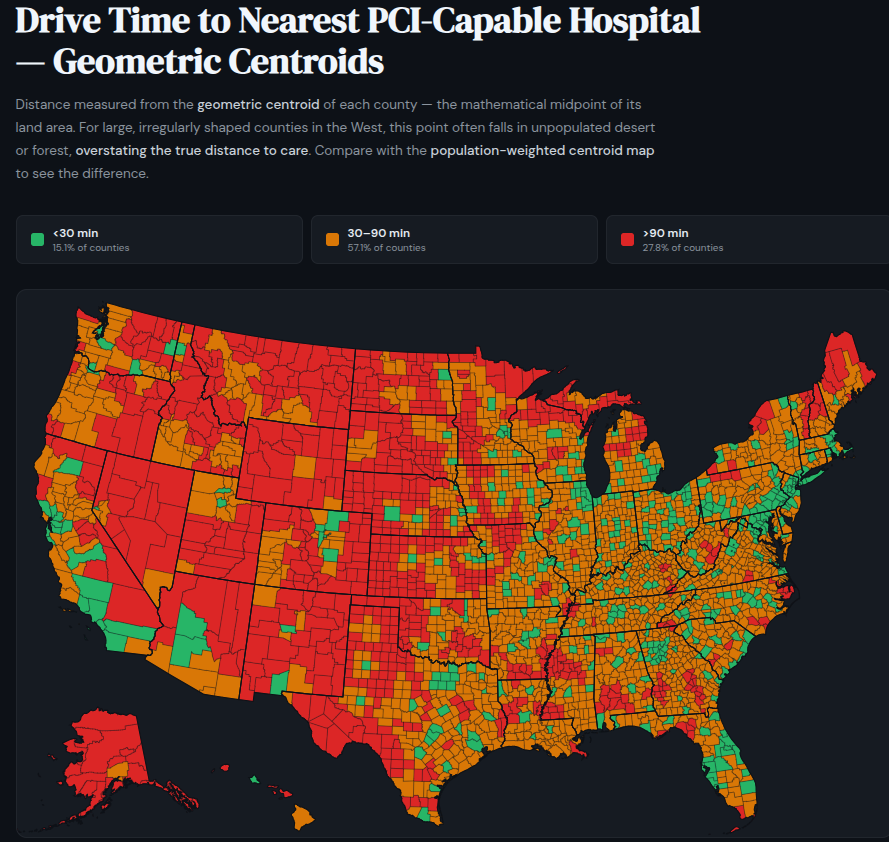
The muse is a 2006 paper by Nallamothu et al. in Circulation — nonetheless probably the most rigorous revealed evaluation of geographic PCI entry in the USA — which discovered that 84% of People dwell inside 60 minutes of a PCI-capable hospital. Utilizing Medicare billing information for DRG codes 246–251 to establish 1,322 hospitals actively performing PCI, and replicating the Nallamothu methodology with up to date information, I discover primarily the identical outcome. No comparable developed nation approaches this degree of entry — and I’ll get to what the closest peer comparisons truly appear to be under.
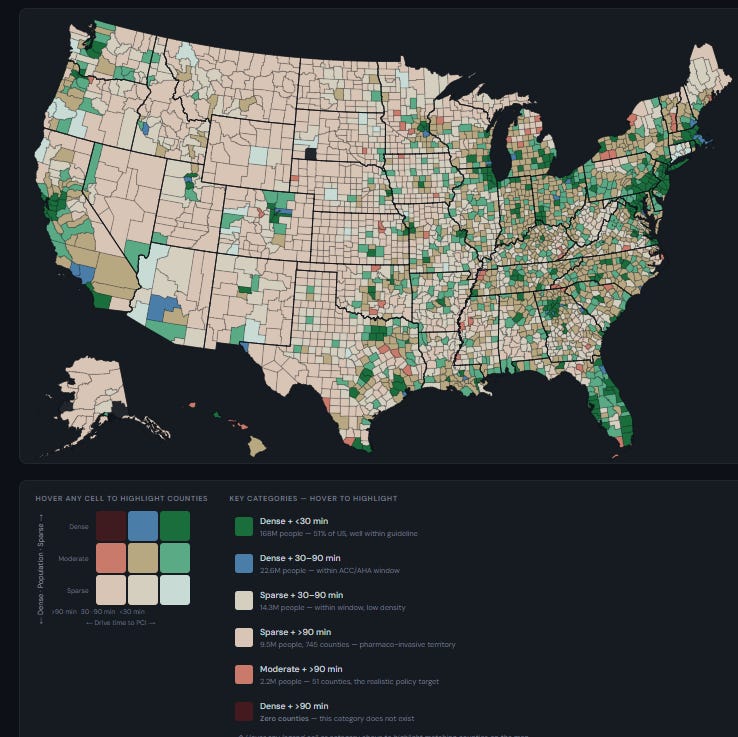
However a easy county choropleth — coloration every county by drive time — has a elementary downside: it treats a county of 600 folks identically to one in every of 600,000. The huge empty counties of the inside West look alarming on the map, and their sheer geographic mass dominates the visible.
The policy-relevant query just isn’t which counties are removed from PCI, however whether or not the individuals who dwell in these counties are removed from PCI — and whether or not the inhabitants density in these areas justifies the type of infrastructure funding the agricultural entry narrative requires.
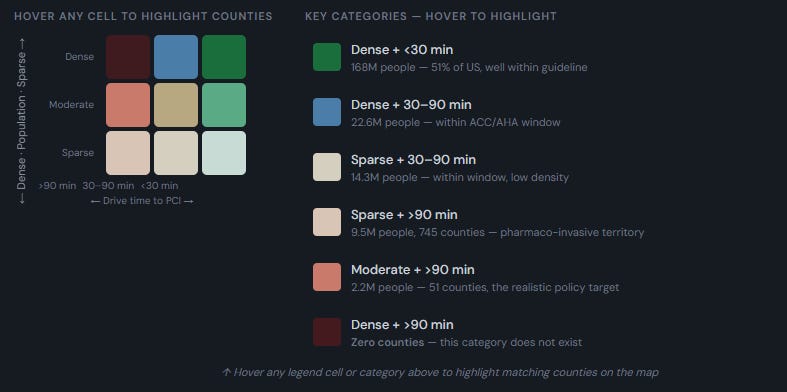
To reply the query I constructed a bivariate map encoding each dimensions, inhabitants density, and distance to a PCI-capable hospital. Counties are assigned to 3 density classes utilizing the fiftieth and ninetieth percentiles of the county density distribution — percentile-based thresholds somewhat than arbitrary absolute cutoffs.

I then outlined three entry bands anchored to the ACC/AHA guideline for opening a blocked artery within the setting of an acute coronary heart assault: inside half-hour, 30 to 90 minutes, and past 90 minutes. Past 90 minutes is a crucial threshold that defines the purpose the place most people could have a cardiac scar or worse if they’re exterior this time window for artery opening.
The centroid downside — and why it issues
Making a database of drive time from a hospital requires defining the place to measure from. The US is separated into counties, and taking the geographic heart of the county (the geographic centroid) as the space to measure from creates some meaningless distortions as a result of the inhabitants in any given county just isn’t essentially clustered in the course of the county. Massive western counties the place almost all of the inhabitants is clustered in a single nook of an enormous space clarify why the easy geographic centroid fails so badly.
Click on on the map to be taken to an interactive map
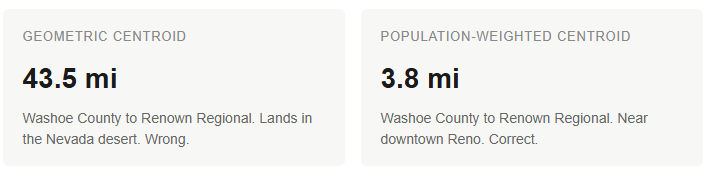
Reno sits within the southwest nook of Washoe County, dwelling to Renown Regional Medical Middle and St. Mary’s Regional. However Washoe County extends a whole bunch of miles into the Nevada desert. Its geometric centroid lands 43.5 miles from Renown, in an space the place primarily no person lives — and an earlier model of a map I made marked it pink. Fortunately, the Census Bureau publishes population-weighted centroids for all 3,143 U.S. counties within the CenPop2020 file, calculated from 2020 block-level information. Washoe’s population-weighted centroid is 3.8 miles from Renown. That’s the appropriate quantity, and so I used population-weighted centroids for each U.S. county.
What the U.S. map truly reveals
The putting discovering just isn’t about dense counties — dense counties cluster round cities, and cities have hospitals. The putting discovering is concerning the reasonable and sparse counties: even at low inhabitants densities, a surprisingly massive share of the American inhabitants is throughout the 90-minute guideline window. However regardless of the big federal equipment devoted to rural healthcare entry, 2.2 million People in moderate-density counties and 9.5 million in sparse counties — roughly 11.7 million complete, or about 3.5% of the inhabitants — dwell past 90 minutes from a PCI hospital. These are the folks the agricultural entry laws is ostensibly constructed for, and after a long time of CAH designations, GME slot carve-outs, Rural Emergency Hospital packages, and billions in cost-based reimbursement, that’s what stays.
Click on on the map for an interactive model
The peer comparability downside — the U.S. is genuinely with out friends
Each worldwide comparability of healthcare entry implicitly assumes the nations being in contrast are meaningfully comparable. They aren’t — at the least not for this query. The US is the third-largest nation on this planet by land space and the third most populous. No high-income democracy comes near combining each. The UK has 68 million folks in an space smaller than Oregon. The Nordic nations collectively have fewer folks than the larger New York metropolitan space unfold throughout a landmass that’s principally accessible by street. These nations face no significant analog to the American geographic entry downside.
The nations that do approximate the U.S. in scale — Russia, China, India, Brazil — fail so comprehensively on PCI entry that no significant comparability is feasible. Russia has maybe 100 PCI facilities for 144 million folks throughout 11 time zones. China’s cath lab infrastructure is closely concentrated in coastal cities. India and Brazil have dramatic urban-rural gradients at a severity that makes rural Nevada look well-served. These should not peer comparators. They’re cautionary tales about what truly occurs when healthcare infrastructure is inadequate at continental scale.
That is why worldwide entry rankings that place the USA alongside Belgium, the Netherlands, and New Zealand should not measuring the identical factor. A rustic the dimensions of Maryland with common insurance coverage and three PCI facilities serving a compact inhabitants just isn’t navigating the identical entry problem as a rustic spanning 4 time zones with 335 million folks. The Commonwealth Fund framework doesn’t account for this, however the bivariate maps do.
Canada: the closest reputable comparability — and a sobering one
Canada is probably the most defensible peer comparability — comparable authorized and institutional custom, comparable earnings degree, bodily adjoining, and regularly invoked by American reform advocates as a mannequin. However making the Canadian map concerned completely different decisions than the U.S. map.
The Canadian map makes use of census divisions somewhat than counties — there are 282 of them, in comparison with 3,143 U.S. counties. PCI heart places had been compiled from CIHI Cardiac Care Quality Indicators and provincial cardiac community directories somewhat than from a Medicare billing equal, as a result of Canada has no public analog to the CMS procedure-level information. The 30 facilities recognized are the very best accessible rely, however the sourcing is much less rigorous than the U.S. method.
Extra importantly, the density thresholds for Canada are calculated individually from Canadian census division percentiles — sparse under 17 per sq. mile, reasonable 17 to 213, dense above 213 — somewhat than making use of U.S. thresholds. Canada is simply so darn sparsely populated total that making use of U.S. density thresholds would classify nearly each Canadian census division as sparse, collapsing the bivariate evaluation right into a single meaningless class. Even with Canada-specific thresholds which are way more forgiving than U.S. ones (what counts as “dense” in Canada could be “reasonable” in the USA) the comparability continues to be stark.
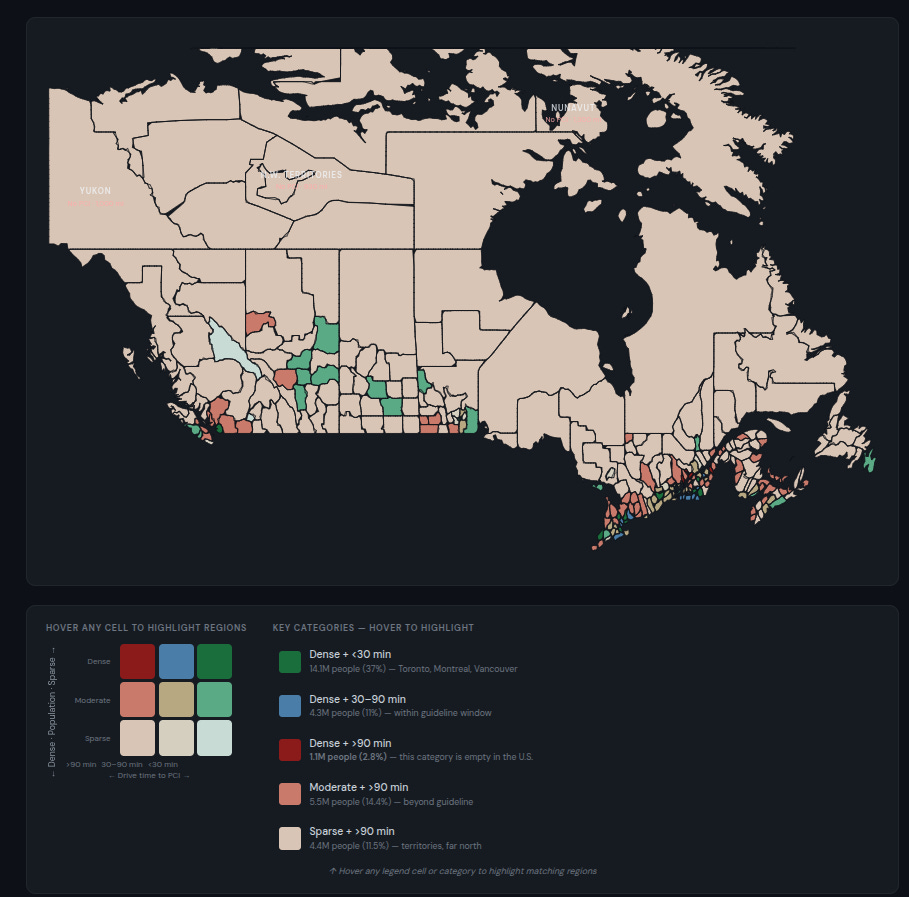
Baber et al. in Open Medicine (2011) discovered that 63.9% of Canadians aged 40 and older dwell inside 60 minutes of a PCI facility, versus 84% of People. That 20-point hole displays a rustic the place 30 PCI facilities serve 38 million folks unfold internationally’s second-largest landmass, concentrated virtually completely inside 125 miles of the U.S. border. Making use of the identical bivariate methodology, roughly 10.9 million Canadians — 28.7% of the entire inhabitants — dwell past 90 minutes from a PCI hospital. That features:
- 4.4 million in sparse census divisions past 90 minutes (11.5% of inhabitants)
- 5.5 million in moderate-density census divisions past 90 minutes (14.4%)
- 1.1 million in dense census divisions past 90 minutes (2.8%) — a class that incorporates zero People
These 1.1 million Canadians in dense-but-far census divisions signify the starkest distinction with the USA. They’re concentrated within the Quebec Metropolis–Trois-Rivières hall — a populated, accessible stretch of southern Quebec that in any cheap sense must be well-served. And but, remarkably, it isn’t.
I manually checked this to ensure the code was appropriate. Listed below are the 4 dense census divisions and their nearest PCI hospitals:
- Francheville (Trois-Rivières space, 452,604 folks): nearest PCI is the Institut universitaire de cardiologie et de pneumologie de Québec — 54.6 miles, estimated 110 minutes
- D’Autray (Berthierville space, 266,948 folks): nearest PCI is the Montreal Heart Institute — 53.4 miles, estimated 108 minutes
- Shawinigan (195,640 folks): nearest PCI is the Institut universitaire de cardiologie — 75.9 miles, estimated 147 minutes
- Montmagny (east of Quebec Metropolis, 150,022 folks): nearest PCI is the Institut universitaire de cardiologie — 47.9 miles, estimated 98 minutes
To place the general numbers in context: the U.S., with almost 9 occasions Canada’s inhabitants, has 11.7 million folks past the 90-minute threshold — 3.5% of its inhabitants. Canada has 10.9 million past the brink out of 38 million — 28.7%. On a per-capita foundation, Canada’s entry hole is roughly eight occasions worse than America’s, in a rustic the place 90% of the inhabitants lives in a slim temperate hall alongside the world’s longest undefended border. A easy framing of American rural entry as a disaster that calls for X whereas holding up Canadian Medicare as a mannequin tells me you’re both uninformed or have a canine within the combat.
So the place does this go away us?
The US just isn’t excellent. Eleven level seven million People dwell past the 90-minute window for emergency cardiac care, and that issues. Each a kind of folks deserves higher. However the trustworthy framing of that quantity is that it represents 3.5% of the inhabitants of a continent-spanning nation — and that no comparable nation on earth comes near matching it. Canada, the nation most regularly held up because the mannequin America ought to comply with, leaves 28.7% of its inhabitants exterior that very same window, together with over 1,000,000 folks in densely populated (by Canada requirements) areas. Rural healthcare entry is a genuinely exhausting downside at continental scale and the headline must be that the USA has solved extra of that downside than anybody else.
And but this isn’t the story you’ll learn within the Commonwealth Fund studies, or within the well being coverage journals, or within the congressional testimony that precedes the following spherical of rural hospital funding. The dominant narrative — that American rural healthcare is in disaster, that we’re falling behind our friends, that the system is failing — is maintained by two teams with aligned incentives. The primary is the tutorial and advocacy class that desires a government-payer system and desires American healthcare to look damaged to justify the overhaul. The Canadian comparability is instructive: the single-payer system they need People to undertake delivers measurably worse geographic entry to emergency cardiac care than the patchwork they need to exchange. The second group is the healthcare trade itself — the well being methods, the hospital associations, the directors of residency coaching packages and the hospitals which are all too joyful to benefit from a Medicare funded program that provides them free doctor labor. All of that is fueled by funding streams that, partially, rely on the continued notion of a rural entry disaster. The Essential Entry Hospital program, the Rural Emergency Hospital designation, the agricultural GME carve-outs: each one in every of these represents cash flowing to establishments, and each try to reform them is met with the identical argument — that any change will shut hospitals and kill sufferers.
The result’s a coverage panorama the place the issue is rarely outlined with actual metrics, the funding is rarely tied to measurable entry outcomes, and the identical establishments that take in billions in rural subsidies additionally foyer aggressively in opposition to significant laws like site-neutral cost reform. Well being methods swallow monumental quantities of federal funding and nonetheless can’t utterly shut the remaining entry gaps. (What they will do, and do very successfully, is drive up the price of care for everybody else.)
There are numerous different levers to tug on if we need to be actually distinctive and enhance rural entry for the 11.7 million People who stay comparatively underserved. I hope I’ve satisfied you that the easy Canadian choice supplied up by many would take us backwards, not ahead. There are some way more wise choices that ought to have extensive public assist.
First, it might appear a better and a greater long run answer to unravel the doctor shortage downside in rural areas by permitting for individuals who develop up in these communities to journey a vastly accelerated path to turning into a basic practitioner. For the time being a vibrant younger child in rural West Virginia is more likely to run his personal HVAC store than run his personal main care observe. Any present main care practitioner will let you know the HVAC route is a a lot smarter and extra profitable path than a path to turning into a doctor that has you spending a minimal of 11 years after graduating from highschool and accruing mid six figures price of debt. It wasn’t all the time that approach — a century in the past, a teen may go from highschool to working towards medication in 5 or 6 years, and lots of of these physicians served precisely these sorts of communities. So Megan and Razib’s touch upon doctor shortages and the necessity for prime expert immigrant labor that isn’t doable to be sourced regionally has a whole lot of layers to it. The “scarcity” is partly a perform of funding a whole lot of residency spots in rural areas, which are then crammed by abroad physicians in search of an entry level to the US well being care system. This framework is a coverage selection that doesn’t even do a very good job of ever fixing the issue as a result of physicians from Lahore and Hyderabad (or their kids, who overwhelmingly go away medication/ select to observe medication in metropolitan areas) solely keep in these communities in the event that they haven’t any different choice. If we, as an illustration, stopped funding rural residency slots, these hospitals which are nonetheless awash in money from a wide range of different federal packages would select completely different labor choices (nurse practitioners/doctor assistants/pay extra to native household observe docs to assist workers sufferers), and all of a sudden you’ll have a really completely different trying panorama of “want” for physicians. Backside line: if you’re going to attempt to engineer one thing — make it extra enticing for native members of the neighborhood to grow to be physicians of their neighborhood somewhat than massively incentivizing rural hospitals to import physicians to fill a necessity that you just created.
Second, if we’re to make use of American tax {dollars} to shut the agricultural entry hole, we have to demand higher outcomes. The information exists to measure, county by county, how far People truly are from emergency cardiac care, main care, and primary surgical providers. Tie funding to some mixture of these measurements. If a rural well being system is receiving cost-based reimbursement, GME coaching slots, and Rural Emergency Hospital subsidies, it must be required to exhibit what entry it’s offering — next-day main care appointments, 24/7 emergency protection, PCI functionality — and lose its designation (and funding) if it can’t.
Third, since we really need extra hospitals, we should always break the monopoly C-suite has on the opening of recent hospitals. The physician hospital ownership ban — a product of the Reasonably priced Care Act, lobbied for by the hospital trade — prevents the folks almost certainly to unravel rural entry issues from doing so. Physicians from rural communities who need to elevate capital, construct amenities, and ship care are legally prohibited from proudly owning the hospitals they’d workers. The ban protects incumbent well being methods from competitors. It does nothing for sufferers. Take into account what occurs the place physicians can personal amenities: Atlas Surgery Center in Amherst, New York — a physician-owned ambulatory surgery center constructed by the neurosurgeons of University at Buffalo Neurosurgery — performs same-day awake endovascular neurosurgery, carotid stenting, Gamma Knife radiosurgery, and sophisticated backbone procedures that will in any other case require multi-day hospital admissions at far larger price. It’s the first ambulatory heart within the nation to supply outpatient Gamma Knife. That’s what doctor possession produces when the regulation permits it. Now think about that mannequin utilized to rural communities that want a hospital and have physicians prepared to construct one. Presently, the regulation says no.
Your complete rural entry debate is premised on the idea that solely massive well being methods backed by federal subsidies can ship care in underserved areas. The proof for that is skinny. What the proof truly reveals is that when physicians are allowed to personal and function amenities — ambulatory surgical procedure facilities, imaging facilities, pressing care networks — they ship care at decrease price with comparable or higher outcomes. Extending that mannequin to hospital possession in underserved areas is probably the most direct path to closing the remaining entry gaps with out the perpetual subsidy machine that has manifestly failed to shut them over three a long time.
The mountain to climb is excessive. Step one would be the hardest: reducing via the noise of motivated lecturers who management many of the messaging on well being coverage and healthcare entry. The general public ought to have a transparent understanding that the disaster narrative they’ve been offered just isn’t an outline of actuality however a product — manufactured by those that revenue from it, whether or not in funding or in political capital. Ought to we attempt to do it even higher? In fact.
However there’s little hope of getting anyplace with out a good grasp of the scope of the issue that faces us.
Anish Koka is a Heart specialist in Philadelphia. He writes on medication and well being coverage on his substack the place this was originally published and likewise cohosts a weekly podcast : The Doctors Lounge
Link to PCI access US/Canada Interactive maps | More on map methodology, limitations